Tech is the ultimate deflationary force of our time.
In 1969, the AGC for the Apollo moon landing had 4 KB of RAM – that was all the compute needed to get Americans to the moon. It cost ~$1,000 per KB to produce (~$8,500 in inflation-adjusted terms). Fast forward, and we’re down to ~$0.00004 per KB – a 75-million-fold price drop.
Yawn, that’s Moore’s Law – transistors on a chip double roughly every two years, at minimal cost increase – and everybody’s heard of it by now.
However, fewer people know its inverse.
Moore’s law backwards
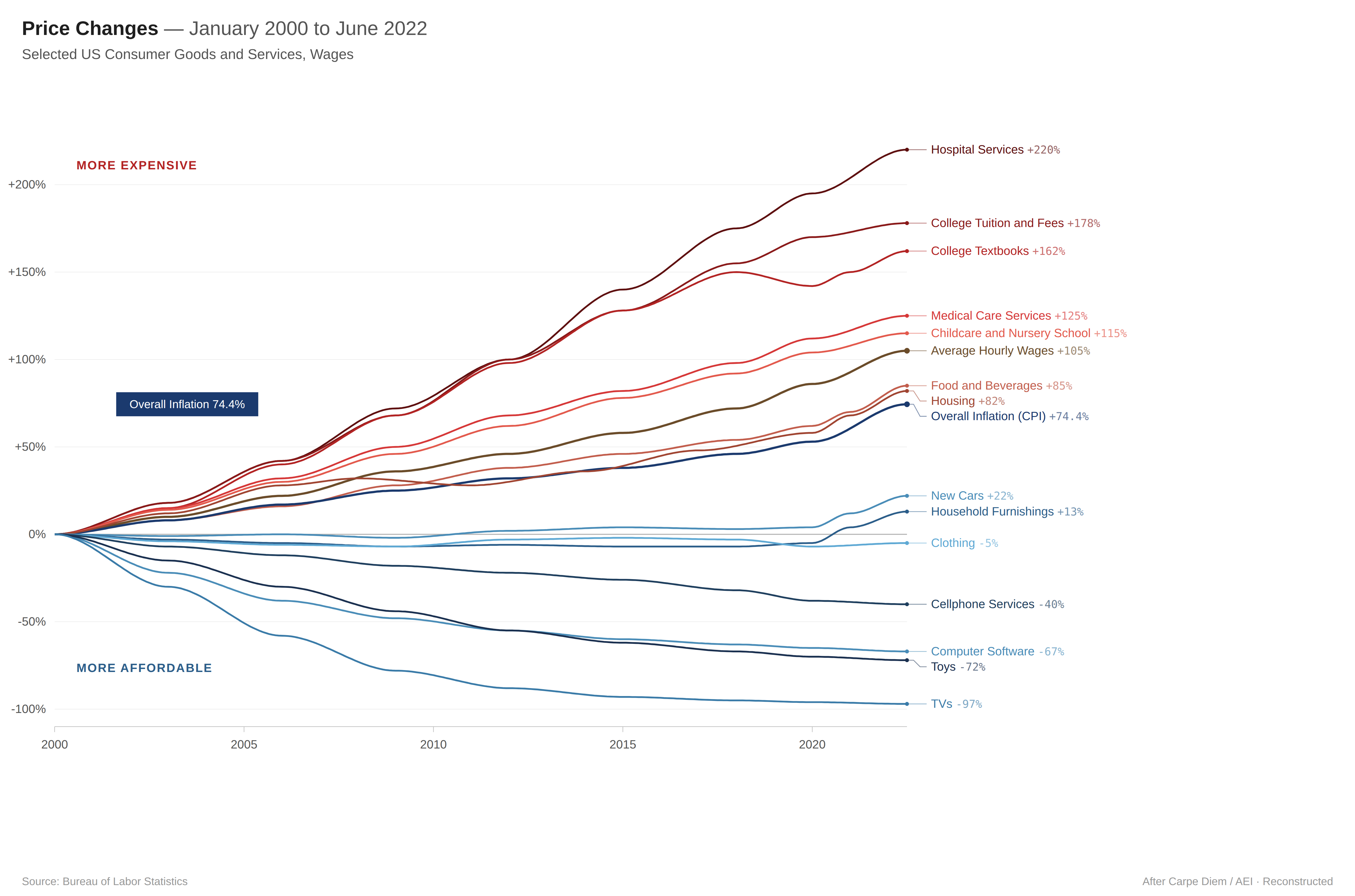
If we look at the graph above, while TVs, smartphones, and software all dropped massively below inflation, some industries massively outpace it. As so often, education and healthcare seem to be the exception.
In 1970, the U.S. spent $353 per person per year on healthcare. In 2024, that number was $15,474 – a 44x increase. That’s more than double what Germany, Japan, and the UK spend per capita. That’s the inverse I was pointing at: Eroom’s Law (Moore’s spelled backwards).
Eroom’s Law states the cost of bringing a new drug to market doubles every nine years. But the underlying dynamic applies more broadly across healthcare: regulatory complexity, risk aversion, and entrenched billing structures compound costs over time instead of driving them down. That’s what happens in regulated industries when no one actively disrupts the cost curve.
Moore’s law for everything
I believe Artificial Intelligence (AI) will be the next great deflationary force. But not in the way software usually works. The old SaaS was software-as-a-service. The new Sa(a)S is service-as-software — replacing labor-intensive services with intelligent systems. Most of what sits above the graph might finally start coming down. But let’s be specific about what this means in healthcare.
In hospitals, labor accounts for over half of total costs. In physician practices, it’s as high as 84%. And yet, physicians spend nearly twice as much time on desk work as on clinical time with patients. Working with physicians and NPs, I see them going from 5 AM to 9 PM every day — split across chart reviews, documentation, and scheduling.
AI doesn’t fix the physician shortage nor does it issue new regulatory reforms, but – given the compounding cost pressures and a shortfall of 86,000 physicians – it can reduce the average labor cost per patient encounter. For a service industry, headcount will always matter.
At first, we’ll see Nurse Practioners, care managers, and office managers being empowered by Amplified Intelligence (AI) and ultimately replaced by true Autonomous Intelligence (AI). Reducing administrative costs matters more than we think. The HMO Act of the 1970s forced insurers to adhere to a 80% Medical Loss Ratio (MLR) which meant they can only spend 20% on adminstriatvie costs. however, all that meant was payers shifting admin costs onto providers by implementing safeguards such as prior auths. Today we see more than 40% of provider budgets going into admin costs.
Human Principles And AI Agents
AI agents are well-suited for administrative tasks. At their core, they are programs that, given a goal, can execute multi-step workflows such as prior authorizations. While full autonomy is often overhyped, most administrative processes can be mapped to deterministic workflows, requiring reasoning only at specific decision points. If a process can be represented in a diagram (e.g., BPMN), it is generally a strong candidate for automation. With advances in computer use, nearly every workflow a practitioner can execute from their desk will become automatable.
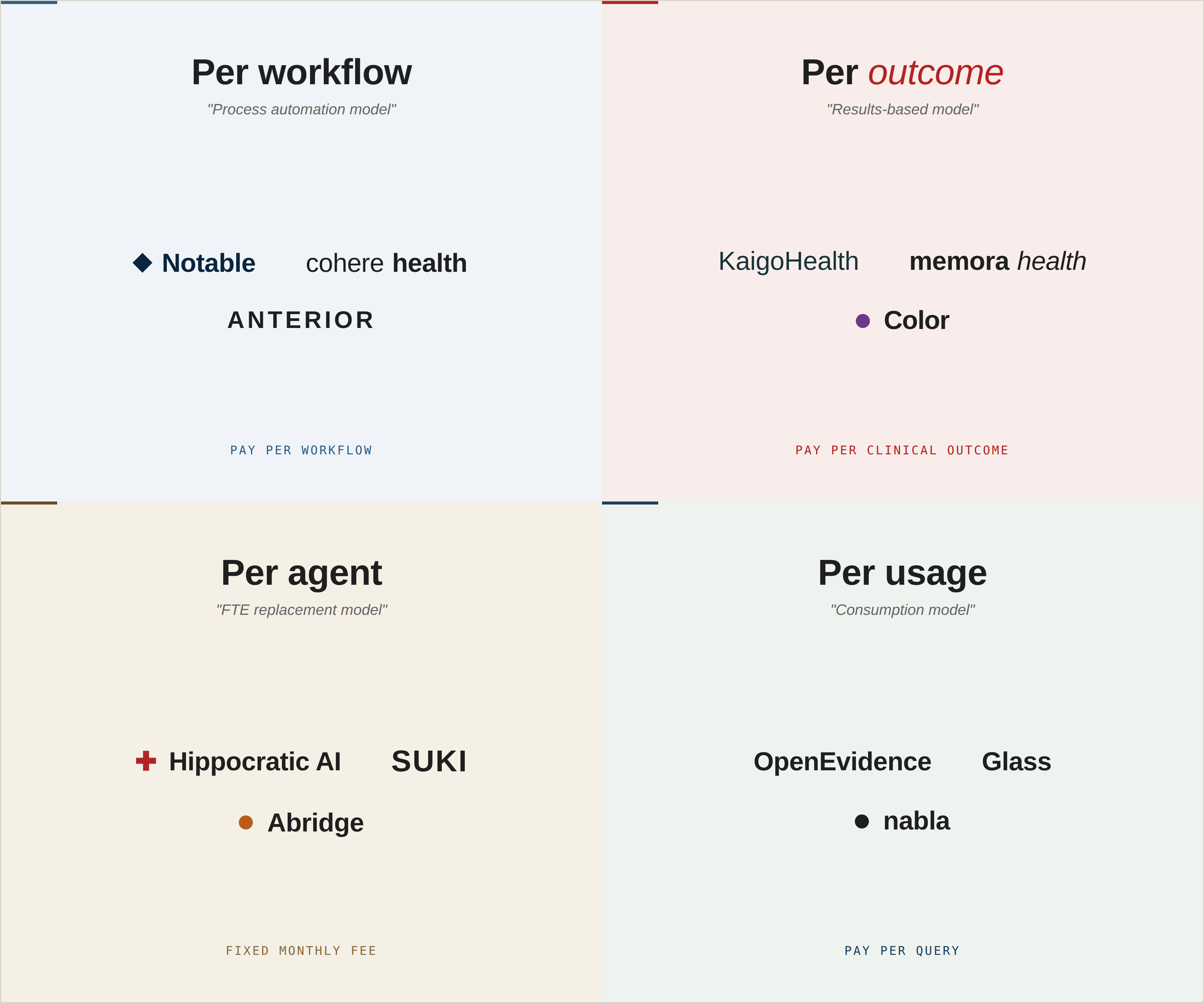
As a service-as-software vendor, there are four primary ways to price AI agents:
1. Per workflow (e.g., per processed claim denial)
2. Per outcome (e.g., reduction in claim denials)
3. Per usage (e.g., number of agent calls)
4. Per agent (e.g., one agent handles up to X tasks per day)
I am particularly excited about outcome-based pricing as it pushes the SaS vendor for efficiency (to maintain steady margins) while not compromising on quality of outcome. Inherently, this also leads to alignment in the principal-agent problem. Literally.
Now, pair outcome-based pricing goals with value-based reimbursement models and you get a both more efficient and effective way of delivering care. Effectively, you create a win-win-win-win relationship:
1. The payer wins, because they save more being charged by value than volume
2. The provider wins, because they improve margins by lowering operational costs while being able to serve more patients
3. The patient wins, because value-based care is inherently aligned with clinical outcomes (e.g. blood pressure or A1c control
4. The vendor wins, because they can operate a service business at marginal costs of zero
This also is my pushback to skimpflation proponents, who basically argue that technology provides products and services at lower costs but by compromising on quality. I wanna go as far as to say quality is fairly objective in healthcare compared to other industries. Take entertainment for instance: Economists claim entertainment got cheaper over the decades. However, what you are effectively comparing is the local theater with a Netflix subscription. Sure, you get to see more movies, but the joy of taking your friends to the theater gets discounted.
When economists claim entertainment got cheaper, they rely on hedonic adjustment – breaking products into features as a proxy for satisfaction. But satisfaction is subjective; what delights one person leaves another cold. Everybody gets to decide for themselves where the theater vs. Netflix example sits.
Back to healthcare, let’s take chronic conditions. There are many clinical studies proving the ideal blood pressure range or A1c score and both are fairly measurable given sufficient patient context. Blood pressure either dropped or it didn’t. HbA1c improved or it didn’t. These are still proxies — but for outcomes that are physiologically beneficial, not merely psychological.
And there’s a structural advantage most people miss. What the internet did for Amazon, AI can do for service industries: access the long tail. Review all charts in an audit, not just a sample. Catch idiosyncratic conditions, not just the obvious ones. Cover all patients, not just the high-risk or highest-revenue. Fewer patients fall through the cracks.
The catch? Under current reimbursement models, none of this efficiency gets rewarded. You still bill Current Procedural Terminology (CPT) codes by time logged or volume of procedures performed. If AI helps a practice see the same patients in less time, the practice earns less. The incentives are backwards.
That’s exactly what makes the next part interesting.
It starts and ends with ACCESS
All of the above is why I’m particularly excited about the CMS ACCESS program. ACCESS stands for Advancing Chronic Care with Effective, Scalable Solutions. It’s a 10-year voluntary model starting July 2026 that introduces Outcome-Aligned Payments – providers get paid for measurable health improvements, not CPT codes or time logged.
Having built CMS-compliant billing infrastructure for CCM and RPM (if you’ve ever tracked 20-minute increments at $42 a pop for billing purposes, you know the pain), the shift to outcome-aligned payments feels like a generational change.
The model targets four clinical tracks covering conditions that affect roughly two-thirds of Medicare fee-for-service beneficiaries:
→ eCKM (Early Cardio-Kidney-Metabolic) — hypertension, dyslipidemia, obesity, prediabetes. Goals: improve BP, lipids, weight.
→ CKM (Cardio-Kidney-Metabolic) — diabetes, chronic kidney disease (stages 3a/3b), atherosclerotic cardiovascular disease. Goals: control BP, lipids, HbA1c. CKD alone accounts for 24% of all Medicare spending.
→ MSK (Musculoskeletal) — chronic musculoskeletal pain. Goals: reduce pain intensity, improve function, opioid-sparing outcomes.
→ BH (Behavioral Health) — depression and anxiety. Goals: symptom reduction measured via validated tools like PHQ-9.
These outcomes are trackable – via BP cuffs, connected devices, patient-reported measures – and the thresholds can be encoded in algorithms.
For me, this is the first step toward an AI doctor that will not only heal the nations people but it’s balance sheet too.
The Healthy Balance Sheet
Why all this matters on a macro scale only becomes apparent when looking at the U.S. balance sheet. More precisely, its footnotes. While many Americans assume the USA is indebted at $39T, that doesn’t fully account for Social Security and… exactly, healthcare via the federal government’s major programs Medicaid and Medicare. What we are actually facing is a fiscal gap in the ballpark of $175T.
As of 2026, the Trump administration with its Big Beautiful Bill tries to aggressively reduce costs in the Medicaid sector. They go the austerity and tax cut route, hoping for incentives to shift toward employment and innovation. While this can be beneficial to AI diffusion — e.g. by creating urgency in the industry — we will also see Emergency Rooms (ER) replacing physician offices, and community health centers and local hospitals closing doors. The cost will be distributed to the insured and the taxpayer.
Better than cutting the budgets would be reducing the costs, which ultimately lowers the budgets needed to serve Medicaid. I believe AI could be a real force of change in healthcare, driving down costs, potentially saving billions, and decelerating debt growth in the United States. That’s the power of deflation.
For now, ACCESS is an experiment. But it could be one of the most consequential ones we’ve seen come out of CMS in a long time.
I hope one day we can take the name literally and AI will give access to cheap healthcare for every American.